
(originally published on February 27, 2026; updated on March 23, 2026)
Table of Contents
- Background
- Methods
- Respondent Characteristics
- Experiences of Stigmatizing Language in Healthcare Settings
- Impact of Stigmatizing Language from Healthcare Providers
- Most Stigmatizing Terms
- Solutions to Decrease Stigma in the Healthcare Setting
- Conclusion
Background
Stigmatizing language in healthcare settings has been widely documented as a barrier to care and contributes to negative health outcomes and well-being among people living with HIV. Language reinforcing stereotypes or implying blame can reduce care engagement, increase internalized stigma, and negatively impact mental health. The Well Project sought to understand the extent to which cisgender and transgender women and nonbinary adults living with HIV experience stigmatizing language and the impact of stigmatizing language on the individual.
Methods
Using a cross-sectional survey design, The Well Project, along with an expert group of advisors*, developed and offered a web-based survey: "Words Matter: The Impact of Language on Healthcare Experiences." The survey consisted of multiple-choice, Likert-scale, ranking, and open-ended response items to obtain quantitative and qualitative data on perceptions of and experiences with stigmatizing HIV-related terms. An IRB-approved cloud-based survey platform was used and tracking of respondents' internet protocol addresses was disabled. Between September 16 and November 11, 2025, the survey was promoted via flyers at events, emails to The Well Project's subscribers and partners, and select listservs. Respondents had to attest that they were ≥ 18 years of age. This analysis is focused on US respondents who self-identified as cisgender women, transgender women, or nonbinary individuals and were living with HIV. Descriptive statistics were used to summarize survey responses using counts and proportions.
Respondent Characteristics
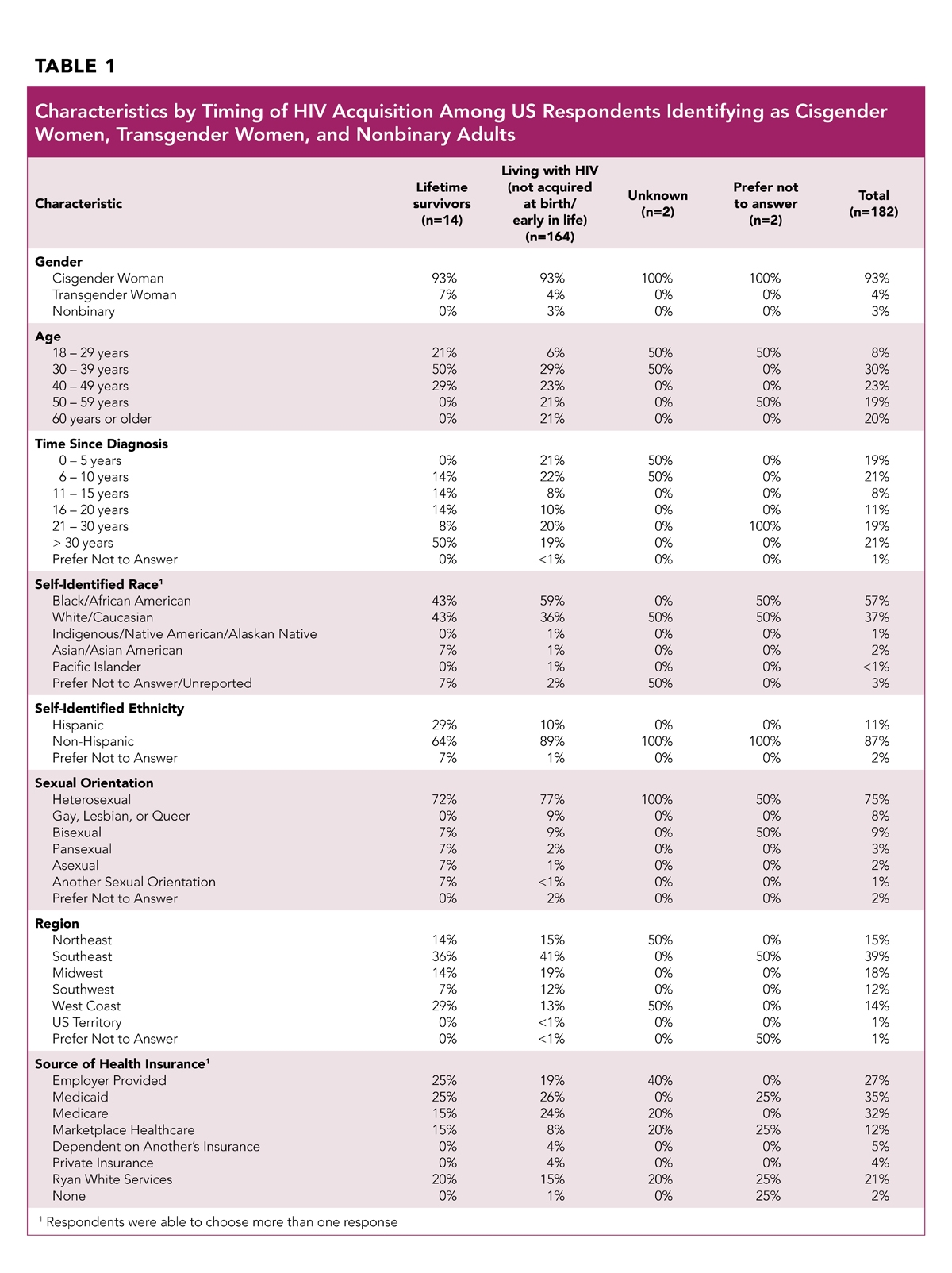
Among 258 total respondents to the survey, 223 (86%) reported being a resident of the United States (US). Among US residents participating in the survey, 182 respondents self-identified as cisgender women (93%), transgender women (4%), and nonbinary adults (3%) living with HIV. These 182 respondents are the subsection on which this report will focus. Characteristics of these respondents are provided in Table 1.
Self-identified lifetime survivors (people who acquired HIV at birth or early in life) account for 8% of respondents; 90% identified as a person living with HIV who did not acquire HIV at birth or early in life; and 2% indicated "unknown" or "prefer not to answer" regarding their HIV acquisition timing. Table 1 outlines the demographic data for lifetime survivors and non-lifetime survivors.
Our sample was diverse in age, with the highest concentration of respondents between the ages of 30-39 (30%), followed by 40-49 (23%), 60 years and older (20%), and 50-59 (19%); 8% reported being between the ages of 18-29.
Respondents also represent a wide range in terms of years living with HIV. Forty percent of respondents reported having lived with HIV for more than two decades; another 40% had been diagnosed within the past decade; and 19% had been living with HIV for 11-20 years (the final 1% indicated "prefer not to answer").
Respondents identified as Black/African American (57%), White/Caucasian (37%), Asian or Pacific Islander (~2%), and Indigenous/Native American (1%); 3% preferred not to answer. Among respondents overall, 11% identified as Hispanic, with a significantly higher rate of lifetime survivors identifying as Hispanic (29%).
Three quarters (75%) of respondents identified as heterosexual; 9% bisexual; 8% gay, lesbian, or queer; 3% pansexual; 2% asexual; 1% another sexual orientation; and 2% preferred not to answer.
Geographically, the greatest percentage of respondents were located in the Southeast US, with the remaining respondents spread fairly equally throughout other regions of the US.
Respondents were queried regarding the type of health insurance they used (and could choose more than one, given that many individuals have multiple sources of insurance). The majority of respondents use Medicaid (35%), Medicare (32%), or employer-provided insurance (27%); 21% access insurance through the Ryan White HIV/AIDS Program, and 12% do so through the marketplace; only 5% reported being dependents on another's healthcare, and 4% reported having private insurance.
Experiences of Stigmatizing Language in Healthcare Settings
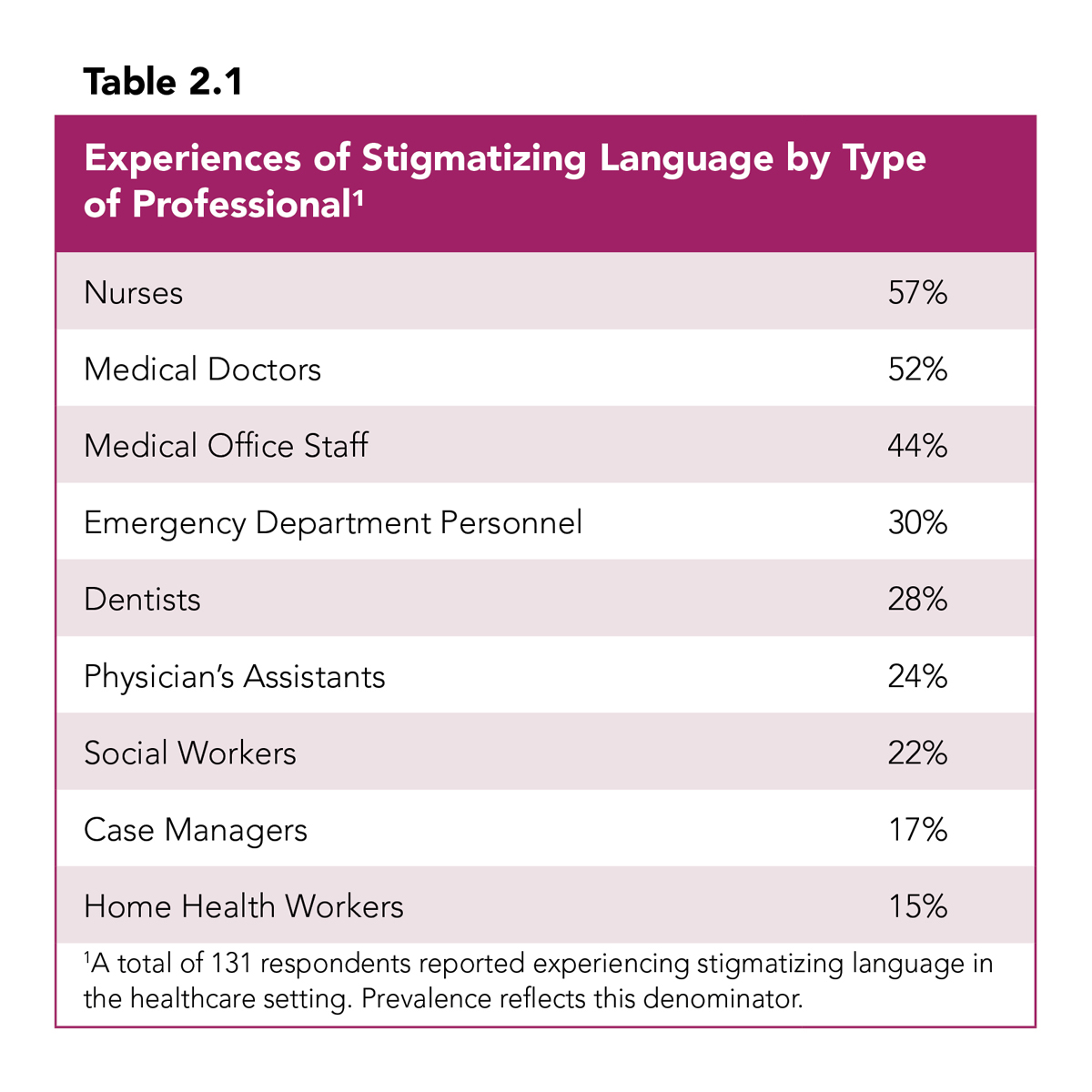
In total, 131 (72%) respondents reported experiencing stigmatizing language in healthcare settings from various healthcare providers and staff (outlined in Table 2.1). The majority of respondents reported experiencing stigmatizing language from nurses (57%) and medical doctors (52%). It is important to also note that 44% of respondents reported experiencing stigmatizing language from medical office staff (which includes front office staff, medical assistants, billing office personnel, and others) - a population in the healthcare workforce who may be overlooked in receiving information and education on person-first language.
"I have had doctors say things like U=U is not backed and she wouldn't support HIV positive patients being in relationships with other people that are not living with HIV. I have also had a Dr say he would not give me a work excuse for attending a Dr appointment with him because we are always trying to manipulate the system. The 'we' was referring to people living with HIV. How am I or we manipulating the system [by] needing to verify we had a legitimate reason to leave work early? That showed me he had biases towards the patients he was providing services to."
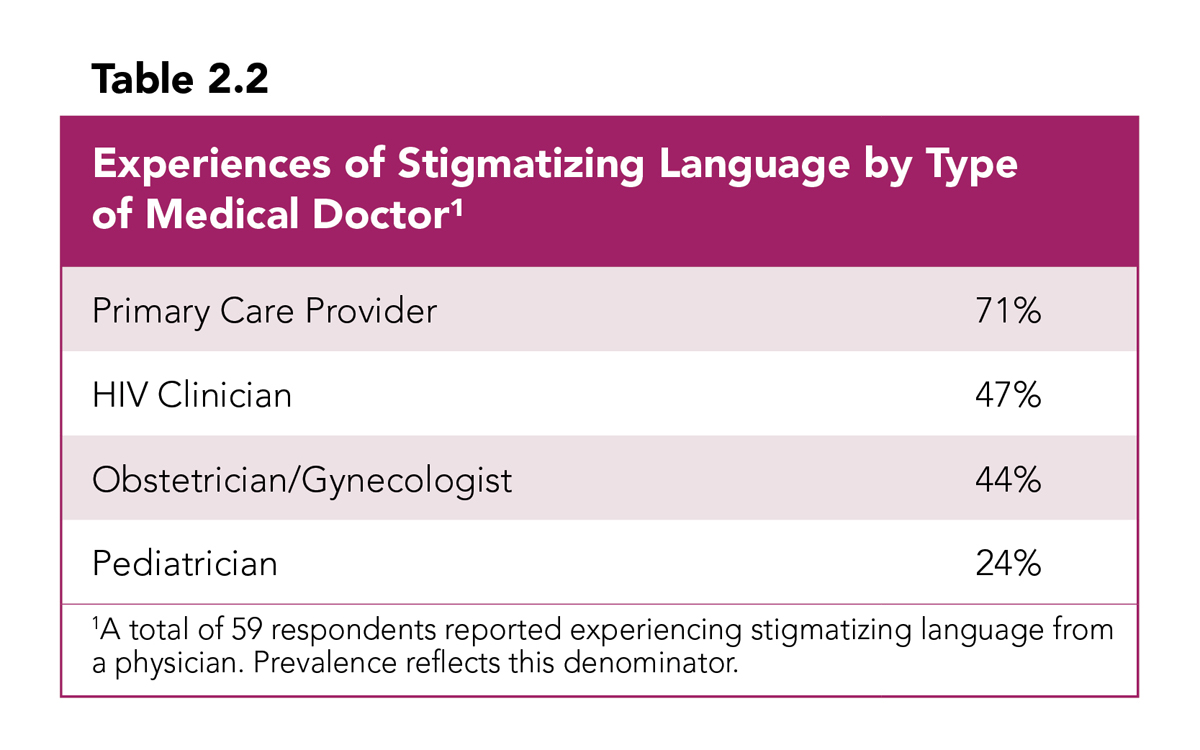
Of the 68 respondents who indicated that they had experienced stigmatizing language from a medical doctor, 59 reported the types of medical doctors from whom they experienced stigmatizing language (Table 2.2). Nearly three quarters (71%) of these respondents reported experiencing stigmatizing language from their primary care provider. These data reaffirm the widespread understanding among HIV advocates of the crucial need for increased HIV education for primary care physicians. Nearly half of respondents also reported experiencing stigmatizing language from their HIV clinician (47%) and/or obstetrician/gynecologist (44%).
"I have seen providers who have been in their role for a long time say stigmatizing language because they have never been corrected. They are not current on the new language and have no interest in learning."
"I was told I shouldn't have more children because I was diagnosed with HIV."
Impact of Stigmatizing Language from Healthcare Providers
For years, The Well Project has been leading efforts to advocate for and create awareness around person-first language among healthcare providers, researchers, media, conference organizers, and community members. This advocacy has been based on decades of anecdotal evidence reported by numerous women who have been negatively impacted by stigmatizing language in healthcare settings. However, calling attention to the impact of stigmatizing language has often failed to restrain its usage among providers and healthcare staff, and imbalanced power dynamics have been evident in their responses (or lack thereof). This research demonstrates the negative consequences on women's healthcare engagement, mental health, and overall well-being across several areas.
"I often hear outdated and fear-based terminology, like 'AIDS victim' or 'clean' used to describe someone who is HIV-negative, which is deeply othering. These words reinforce a harmful 'us vs. them' dynamic in a space that should be defined by safety and clinical accuracy."
"I encounter assumptions that my gender is directly tied to my status, such as being called 'promiscuous' or having my sexual history scrutinized more heavily than a man's. This language reinforces harmful stereotypes that place moral judgment on me rather than focusing on clinical care and support. It makes the healthcare environment feel dismissive and judgmental."
Among 131 respondents who reported on the impact of stigmatizing language:

85 (65%) reported that the use of stigmatizing language from a healthcare provider impacted their self-esteem and mental health
"Hearing stigmatizing language from a healthcare provider, someone who is supposed to be a source of support, is uniquely damaging. It can internalize shame, making me feel defined by my status and 'less than' others. It directly undermines my self-worth and can lead to increased anxiety, depression, and isolation."
71 (54%) reported delaying, avoiding, or missing healthcare appointments as a result
"There have been times when the dread of encountering a specific provider's judgmental tone or being subjected to awkward, stigmatizing questions made me reschedule an appointment. The mental and emotional energy required to prepare for potential stigma is exhausting. It creates a barrier where the short-term relief of avoiding a negative interaction feels heavier than the long-term benefit of the appointment, leading to delays in seeking care."
68 (52%) reported effects on their overall well-being or quality of life
"[Stigmatizing language at least partially] led to the use of substances for quite some time. ... How I was treated affected my mental health and made me feel useless and disgusting."
51 (39%) reported finding it difficult to take antiretroviral medication
"There were times when harsh words from providers made me lose motivation to stay consistent with my treatment."
"I've encountered language and assumptions that directly tie my HIV status to my socioeconomic class. Staff have made automatic presumptions about my financial instability, housing situation, or level of education without any basis. For instance, I've been preemptively routed to social services for housing or food assistance without being asked if I needed them, based solely on my status. This use of overly simplistic, condescending language and these blanket assumptions feel dismissive, as if I am a stereotype rather than an individual. It creates a significant barrier to trust and open communication, making the healthcare environment feel judgmental instead of supportive."
Most Stigmatizing Terms
Throughout their lives, women may experience multiple forms of oppression and discrimination based on gender, race, sexual identity, socioeconomic status, or other factors. These conditions are often reinforced through language. Over the years, repeatedly hearing language that perpetuates stigma, oppression, and discrimination ultimately affects the health and well-being of women diagnosed with HIV, as described above.
For more information about the importance of language and a list of preferred terms by HIV community members (which is always evolving and regularly updated), visit our fact sheet, Why Language Matters: Facing HIV Stigma in Our Own Words.
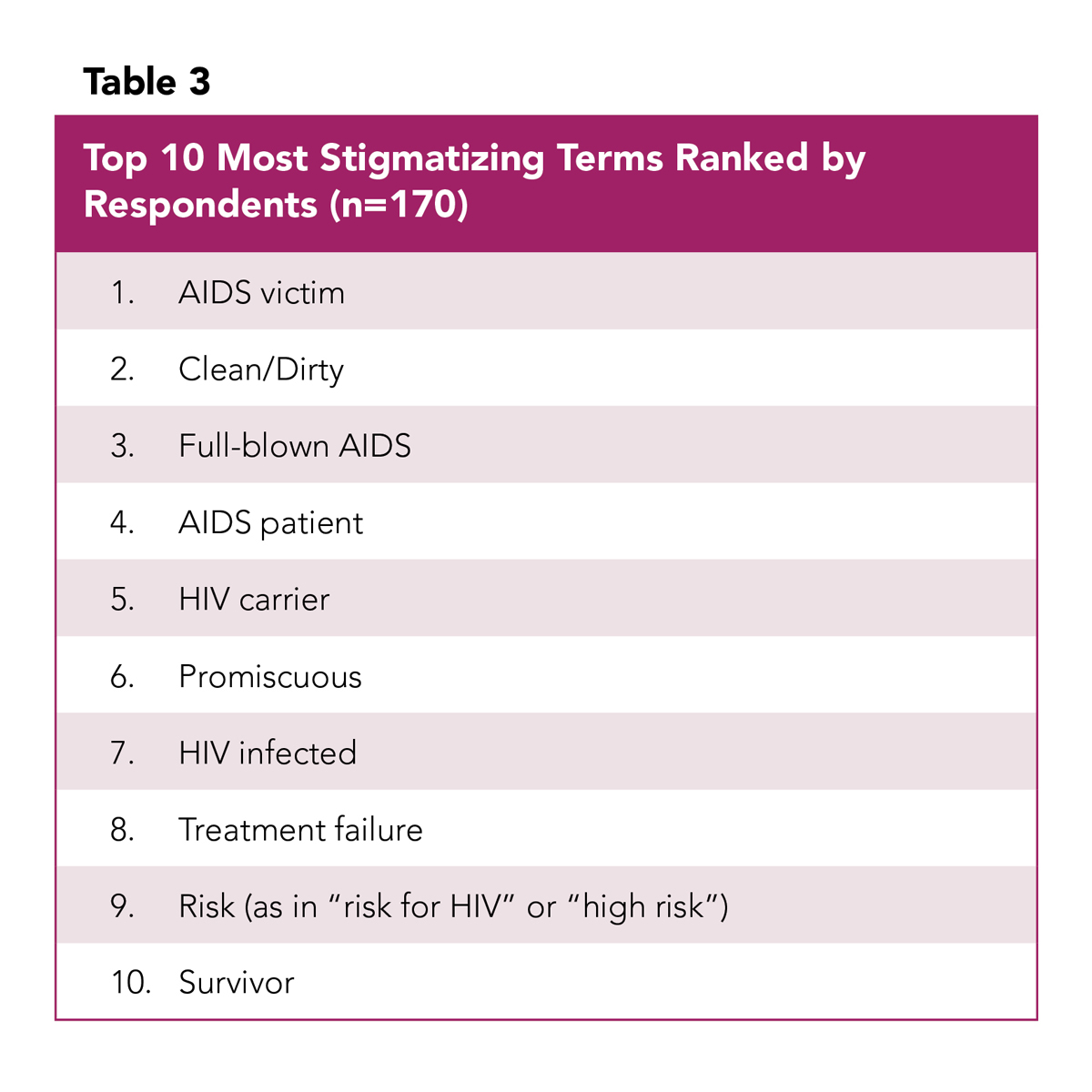
Respondents were asked to rank specific terms using a scale of "Not at all stigmatizing"; "Slightly stigmatizing"; "Neutral"; "Moderately stigmatizing"; or "Very stigmatizing." Table 3 shows the ranking of the top ten most stigmatizing terms (reported as "very stigmatizing" and "moderately stigmatizing") identified by respondents.
Respondents were also asked to categorize the frequency with which they encountered these terms. Among the top ten terms deemed to be most stigmatizing, "risk," "HIV infected," and "survivor" were the most frequently encountered terms by respondents. It is also important to highlight that regional differences were noted in the frequency of use of these terms. For example, respondents from the West Coast reported the highest frequency of encountering the term "risk" compared to all other regions. Individuals in the Southwest and West Coast regions reported encountering the term "HIV infected" more frequently than the other regions of the country, and individuals in the Northeast reported more frequently encountering the term "survivor" compared to all other regions of the country.
Respondents were asked (if they felt comfortable doing so) to share an example or description of stigmatizing language they experienced in a healthcare setting. Forty comments were shared; below are a select few:
- "Sometimes, a healthcare provider has used terms like 'HIV-infected person' in a way that made me feel like my condition defined me, rather than focusing on my overall health. Other times, casual questions about my lifestyle felt judgmental, even if unintentional."
- "I have been asked if I was a drug addict or prostitute, regarding how I contracted HIV"
- "Dentist asking about ever having 'full-blown AIDS'"
- 'When I was pregnant I was labeled as [a] high-risk patient because I was born positive. I didn't understand why I was labeled that when I had been undetectable all my life. I asked a provider and they stated it was labeled that because I am living with HIV."
- "Walking down the hall in the clinic and overhearing one nurse tell the other to make sure you wipe down the table in bleach. She's HIV."
- "I went to emergency room because food poisoning they had young trainees out of school treating and they snickered, whispered, laugh and threw me in a room at the back end of ER as if I was going to contaminate the whole staff"
- "HIV carrier. 'Get the dental equipment for carriers so we don't infect others. These are your medications we store them differently since they're for carriers'"
- "Nurse crying hysterically and getting staff accusing me of infecting my baby with HIV whilst breastfeeding in the USC/LAC hospital, ultimately adding to the allegations against me as a mother that led to the removal of my child."
Solutions to Decrease Stigma in the Healthcare Setting
Using inappropriate language to describe HIV and women increases the amount of stigma and stress women experience daily. One way to address stigma is to use person-first language. Person-first language puts the person before the illness or label and describes who they are, not what they have been diagnosed with. Person-first language helps eliminate prejudice and removes value judgments. When we describe people by labels or medical diagnoses, we devalue and disrespect them as individuals. Person-first language respects people for who they are.
When asked if person-first language improves communication and reduces stigma, out of 166 respondents, 130 (77%) agreed.
Respondents were asked What types of support would you like to see more of to address HIV-related stigma? and were asked to rank their top three choices among five areas. In order of priority, below are the ranked responses:
- Education and awareness campaigns
- Training for healthcare providers to reduce stigma
- More support groups for women living with HIV
- Legal protections against discrimination and criminalization
- Counseling and mental health resources
This research clearly demonstrates a continuing and urgent need to increase education and awareness around person-first language, including among healthcare providers.
When asked to comment on providers' use of person-first language and how to improve interactions with providers, there were more than 50 responses. Below are selections from these responses:
- "[Person-first language] makes me feel like a whole person, not just defined by HIV. Saying a woman living with HIV acknowledges my humanity and dignity."
- "HIV-infected woman is stigmatizing; the word infected changes everything vs. woman living with."
- "Doctors and nurses should avoid labels like non-compliant or 'risky' and instead use supportive language such as 'working on adherence' or 'support needed.' This would show empathy in their tone and words which makes a big difference."
- "I would appreciate providers using people-first language consistently, avoiding terms that imply blame or moral judgment, and focusing on supportive, neutral, and factual language. Additionally, asking respectful questions about lifestyle or identity without assumptions would make interactions feel safer and more comfortable."
- "Using people-first language emphasizes the person rather than the condition. It helps healthcare providers focus on the individual's overall health and reduces the feeling of being labeled or judged."
- "People-first language is crucial because it separates my identity from my diagnosis. I am a person first; the virus is a health condition I manage, not my defining characteristic. Phrases like 'HIV-infected woman' make me feel like a contaminated object or a walking diagnosis. In contrast, 'woman living with HIV' acknowledges my humanity first. This small shift in phrasing is a fundamental sign of respect from a provider. It directly reduces stigma by refusing to label me as the disease and fosters a more collaborative, person-centered partnership in the exam room, which is the foundation of effective healthcare."
Respondents were also asked How effective are the following strategies in helping you manage HIV-related stigma? We calculated a weighted average response to each coping strategy, assigning a point of 1 to "Not at all effective"; 2 to "A little effective"; 3 to "Somewhat effective"; and 4 to "Very effective" and dividing by the total number of individuals who provided one of these responses. No points were assigned if a respondent provided a response of "I don't use this," and these responses were not included in the weighted average calculation.
The Well Project encourages allies in the healthcare and research sectors to help "call in" their peers when stigmatizing language is utilized, to lessen the burden on community members and other advocates to do so - especially in settings where community members are not adequately represented.
Below are the top five coping strategies as reported by respondents ranked from the most effective to the least effective:
- Practicing self-acceptance and self-care
- Educational training and resources for friends and family of women with HIV
- Speaking out against stigma or educating others
- Connecting with other women living with HIV
- Joining support groups or community organizations
Practicing self-acceptance and self-care was ranked highest by respondents and highlights the need for healthcare provider training and educational initiatives emphasizing holistic care for people living with HIV, particularly for those who are newly diagnosed.
Conclusion
Since the beginning of the epidemic, people living with HIV have demanded the use of respectful language when it comes to their diagnosis. The Denver Principles were written by HIV advocates in 1983, in the very early days of the epidemic. In its opening words, the Denver Principles called for the use of respectful person-first language:
"We condemn attempts to label us as 'victims', a term which implies defeat, and we are only occasionally 'patients', a term which implies passivity, helplessness, and dependence upon the care of others. We are 'People With AIDS.'"
There have been many evolutions of preferred terminology (and it will continue to evolve), but many healthcare providers, researchers, and others who interact with and/or describe people living with HIV have not understood the impact or importance of language.
While our report focuses on the experiences of cisgender women, transgender women, and nonbinary adults (because we center these underrepresented populations in our work), this research is important across all populations living with HIV.
The Well Project undertook research to build upon anecdotal evidence with quantifiable data that will ultimately raise awareness of the impact of language. This research demonstrates that the use of stigmatizing language can have a negative effect not only on mental health, self-esteem, and quality of life, but also on an individual's willingness to go to their healthcare appointments and take their medications as prescribed.
While it is important to note that nurses and medical doctors were among the most frequent to use stigmatizing language, training of medical office staff represents another opportunity to ensure that interactions with people living with HIV are respectful and non-stigmatizing. Primary care providers ranked at the top of the list of using stigmatizing language (71%) in the healthcare sector; but HIV clinicians, who should receive frequent training and education on cultural relevance, also had a high frequency of using stigmatizing language (47%), as did OB/GYNs (44%).
There is a clear need, underscored by respondents in this research project, for improved education and training around person-first language (both overall and for healthcare professionals) that could have a positive impact on their overall lives and interactions with their providers and others. We would like to acknowledge the community members, clinicians, researchers, and others who have been at the forefront advocating for and implementing person-first language. The Well Project encourages allies in the healthcare and research sectors to help "call in" their peers when stigmatizing language is utilized, to lessen the burden on community members and other advocates to do so - especially in settings where community members are not adequately represented.
We look forward to providing additional data from this important research in the future.
Expert Advisory team:
- Kimberly Canady, BS
- Founder, Conversations with Kim, LLC
- Community advisory board member, The Well Project
- Aryah Lester
- Board of directors secretary, The Well Project
- Vickie Lynn, PhD, MPH, MSW
- Assistant professor of instruction; MSW program chair, face-to-face; interim online MSW program chair, School of Social Work, College of Behavioral & Community Sciences, University of South Florida
- Person living with HIV (40+ years)
- Kate Powis, MD, MPH, MBA
- Massachusetts General Hospital
- Harvard Medical School
- Harvard T.H. Chan School of Public Health
This program is supported through a grant from Merck.


